Surgery is used at different times in treatment. Sometimes, surgery is at the beginning and other times surgery is used after the tumour has been shrunk with other treatments. Also, the type of surgery and amount of breast tissue that is removed will depend on the type, size, and location of your cancer.
Your surgeon will review your options with you and help you make a plan that’s right for you.
The common types of breast cancer surgery are:
- breast-conserving surgery (also called lumpectomy, segmental resection, partial mastectomy, wide excision or wedge resection)
- mastectomy
- mastectomy with immediate reconstruction
Most of the time these surgeries also include removing some of the lymph nodes under the arm on the same side as the breast cancer surgery.
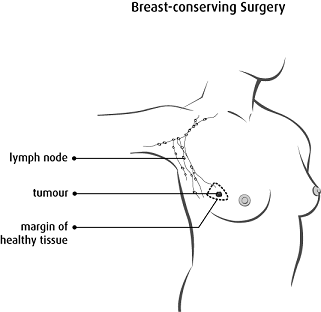
Breast-conserving surgery
The goal of this surgery is to keep as much normal breast tissue as possible. If the cancer is not too big, this surgery may be used.
Breast-conserving surgery is also called:
- lumpectomy
- segmental resection
- partial mastectomy
- wide excision
- wedge resection
For this surgery, your breast tissue with cancer is removed, along with a small amount of healthy tissue around it, called the margin. Your incision (cut) is closed with stitches or staples. The stitches are usually dissolvable, so you won’t need them removed.
You may have heard the term oncoplastic surgery. This type of surgery uses reconstructive techniques to shape the remaining tissue or form a new breast.
Oncoplastic surgery may be simple, such as hiding a scar and rearranging the breast tissue to fill the gap created by the lumpectomy (“Level I”), or more complex, such as combining a traditional lift and reduction with the tumour removal (“Level II”).
Depending on what you need and the training of the surgeon, this may be done by your breast surgeon on their own, or together with a plastic/reconstructive surgeon.
Copyright © 2017 Canadian Cancer Society. Graphic used with permission.
The tissue that has been removed will be sent to a lab for the pathologist to make sure your margins are free of cancer. If your margin contains cancer cells, it is called a positive margin. In this case, your surgeon will have to remove more tissue using the same incision site, at a follow-up surgery. This is called a re-excision.
Mastectomy
Sometimes the surgeon must remove all of your breast tissue. This is called a mastectomy. It can be done as a total mastectomy or a modified radical mastectomy.
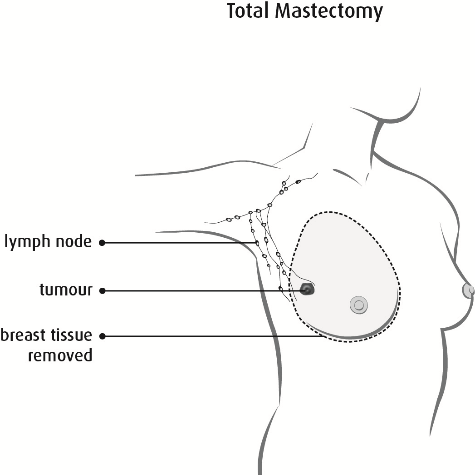
Total mastectomy
Copyright © 2017 Canadian Cancer Society. Graphic used with permission.
A total mastectomy (simple mastectomy) is when the surgeon removes all of your breast tissue. A
sentinel lymph node biopsy may be included with this surgery.
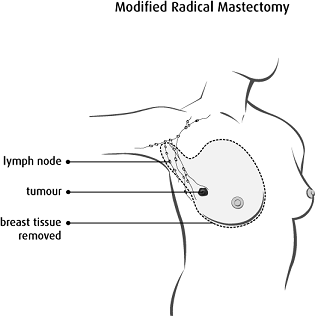
Modified radical mastectomy
Copyright © 2017 Canadian Cancer Society. Graphic used with permission.
A modified radical mastectomy is when some parts of your breast are removed. Usually the surgeon removes:
- all of your breast tissue on the affected side
- the lower 2/3 of the lymph nodes in the armpit (axilla) of the affected side
When you have both breasts removed, it is called a double or bilateral mastectomy.
Lymph node surgeries
Lymph nodes are small glands that are found in groups throughout your body. Lymph nodes are connected by lymph vessels. Breast lymph vessels bring fluid from your breast and arm to the lymph nodes at the collarbone and armpit (axilla).
The lymph nodes filter this fluid to remove bacteria, viruses, and cancer cells. If breast cancer spreads, it will most often spread to lymph nodes in your armpit before the cancer spreads to other parts of your body.
Lymph node surgery is done for 2 reasons:
Sometimes, a person has both surgeries. Your surgeon will talk to you about which surgery is right for you.

Copyright © 2017 Canadian Cancer Society. Graphic used with permission.
Sentinel lymph node biopsy
The sentinel lymph nodes are the first nodes where breast cancer will travel as it spreads. Usually if the sentinel lymph nodes are cancer free, then it means the other axillary lymph nodes probably don’t have cancer cells either.
How it works
A special dye made of a radioactive tracing material (tracer) is injected into the breast near your areola (the dark skin around your nipple). This tracer follows your lymph system, just as your cancer can, and provides a map of where your sentinel nodes are in your breast. The tracer doesn’t tell whether or not there is cancer in the lymph nodes. It just shows the surgeon where the lymph nodes are.
Where do I get the tracer?
You’ll have this sentinel lymph node mapping either the day before your surgery or the morning of your surgery at the Nuclear Medicine Department or Diagnostic Imaging Centre. You may feel uncomfortable when the radioactive tracing material is injected into your breast.
What happens during surgery?
Your surgeon:
- will use a scanner to find the sentinel lymph nodes.
- may also inject a blue dye (in addition to the tracer). This will color the sentinel nodes blue and make them easier to find.
If blue dye is used, it will turn your urine (pee) green for about 24 hours. The dye may also cause the skin of your breast to change colour in the area where the injection was done. This change in colour could last for months.
Your surgeon will then remove the sentinel node(s). The sentinel lymph nodes are sent to the lab where a pathologist will test them for cancer.
When the surgery is done the tracer leaves your body through your urine. Remember:
- It’s important to always wash your hands very well after using the bathroom. This removes any traces of radioactivity.
- The amount of radiation in your body is not dangerous and will disappear quickly. You can still have contact with other people.
Your surgeon will need all of the information about your tumour and lymph nodes before deciding if you need more surgery on your lymph nodes.
Please be patient. The report from the pathologist can take up to 14 days. The test results are reported as positive or negative for cancer. Positive means cancer was found. Negative means no cancer was found. The results will help your doctors determine the stage of your cancer and the best treatment plan for you.
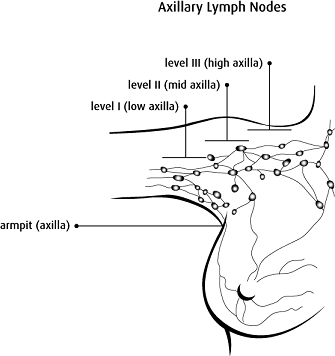
Axillary lymph node dissection
The axillary lymph node dissection may be done when cancer has spread in the lymph nodes.
If you have an axillary lymph node dissection, your surgeon will remove many lymph nodes from under your arm. Your surgeon will place a drain into the area after the lymph nodes are removed.
A pathologist examines the lymph nodes for cancer cells. The test results are reported as positive or negative for cancer. The results will help your doctors decide the stage of your cancer and work with you to determine the best treatment plan for you.
You may need radiation or systemic treatment after this procedure to kill any cancer cells that cannot be seen.
Copyright © 2017 Canadian Cancer Society. Graphic used with permission.
Visit
MyPathologyReport.ca to learn more about what your results mean.
Breast reconstruction surgery
Breast reconstruction means rebuilding the breast using either breast implants or tissue from other parts of your body. This surgery is sometimes done:
- immediately (at the same time of the cancer removal) or
- delayed (months to years after mastectomy)
Talk to your surgeon to see if and when breast reconstruction is right for you. If now is not the right time, you can always consider it in the future when your cancer treatment is finished.
Your breast reconstruction surgery will be done by one or more surgeons. In Alberta, breast reconstruction surgery is considered part of your overall breast cancer treatment. Alberta Healthcare covers the cost of breast reconstruction.
Your options for reconstruction surgery will depend on:
- Your cancer site, stage, and grade.
- How much breast tissue needs to be removed.
- Your health right now.
- Your need for other treatment after surgery, such as radiation. Reconstruction surgery is more risky in people who smoke, have a high body mass index (BMI), or other serious medical problems, because there’s a high risk of problems (complications) from surgery.
- Your personal choice.
With any surgery, there are benefits and risks. Your healthcare team will work with you to help you make a decision that is right for you.
If you are having reconstruction surgery, you will have either breast implants or an autologous reconstruction.
Breast implants
Some people choose to have breast implants after mastectomy. Breast implants are silicone sacs filled with either saline (salt solution) or silicone gel. The implant is usually placed just behind the chest muscle.
In situations where breast skin had to be removed, or where you would like a larger breast than you had before, an expander will be used. The expander will help stretch the skin and create the space the implant will need. Here are some general options:
-
1 stage (1 surgery) - Option A: permanent implant. Sometimes you don’t need a tissue expander. A breast implant may be placed during your mastectomy surgery using a special mesh to make a space under your chest muscle. The size of the implant is chosen before surgery.
-
1 stage (1 surgery) - Option B: expander-implant. An “expander-implant” with a special removable port will be placed. Your surgeon can add small amounts of saline over the next few months in clinic. This allows the skin around the implant to stretch slowly over time. Once the right size is reached only the injection port will be removed, with the implant left in place permanently. There are different types of expander-implants, some with only saline, some with combinations of saline and silicone.
-
2 stage (2 surgeries). Your surgeon will place an “expander.” Approximately every 2 weeks they will add a small amount of saline through a built-in injection port. This will allow the skin around the expander to stretch slowly. This usually takes 1-3 months. Once the skin has stretched enough and the “pocket” holding the implant is the right size, you will have a second surgery. Your surgeon will remove the expander and place a permanent implant. You cannot have an MRI while the expander is in place.
Visit the
Canadian Breast Cancer Network for more detailed information on implants and other reconstruction surgery options.
Autologous breast reconstruction (reconstructed with your own tissue)
When your surgeon uses tissue from other places in your body to recreate a breast, it’s called autologous breast reconstruction. There are many different ways a surgeon can do this. Your surgeon will talk with you about what they recommend for you.
The tissue they remove to reconstruct your breast is called the flap. There are 2 main considerations for the procedure:
1. Common donor sites (area of the body the flap is removed from)
- Stomach (abdomen)
- Back flap (latissimus dorsi)
- Buttocks (gluteus)
- Inner thigh (upper gracilis)
Using tissue from the abdomen is the most common. But, sometimes this is not recommended, such as when you:
- do not have tissue from your abdomen to use, or
- had abdominal surgery in the past.
2. Blood supply to the flap (attached or free)
-
Free flap: The tissue is completely detached from the donor site and reconnected to the blood vessels in the chest area. Common free donor sites: abdomen (transverse rectus abdominis (TRAM) or deep inferior epigastric perforators (DIEP))
-
Attached (pedicled) flap: The tissue stays connected to some of the blood vessels at the donor site. The tissue is moved under the skin to your breast area. Common attached donor sites: abdomen (Pedicled TRAM) or back (Latissimus or thoracodorsal artery perforator (TAP))